A Lesson From COVID-19: A History of Racism and Disease in Hawai‘i
As someone of Chinese descent who lives in the multicultural mixing pot that is Hawai‘i, I find myself thinking about the fact that May is Asian and Pacific Islander (API) Heritage Month, and how the opportunity to reflect on API heritage in the United States could not have come at a better time. In some ways, what’s happening today with COVID-19 is history repeating itself. As the disease has spread, there has also been a rise in anti-Asian sentiment and xenophobic attacks on Asian people throughout the country. These attacks are provoked and encouraged by the dangerous and inaccurate rhetoric spewed by the current administration, such as referring to COVID-19 as “the Chinese flu.”
Disease outbreaks have long been racialized throughout history and used to systemically scapegoat certain groups of people. This panic-fueled racism intersects with other systems of oppression, such as incarceration, white supremacy, colonization, and poverty.
Although the anti-Asian sentiment on the mainland has been more extreme, we’re still experiencing traces of it here in Hawai‘i, the state that boasts the largest percentage of Asian and Native Hawaiian and Pacific Islander populations thanks to a unique history of plantation labor immigration from Asia and Western colonization. In fact, Hawai‘i’s history of discrimination against API people is one we can learn from.
When the first COVID-19 cases in Hawai‘i were confirmed in early March, Honolulu’s Chinatown saw an immediate 50 percent drop in business. The once bustling streets were suddenly silent and empty, while the malls continued to draw in large crowds. Around this time, a friend confided in me about how she feared for the security of her mom’s job as a waitress in a Chinese restaurant in Honolulu. The restaurant was losing customers, and her mom was losing shifts.
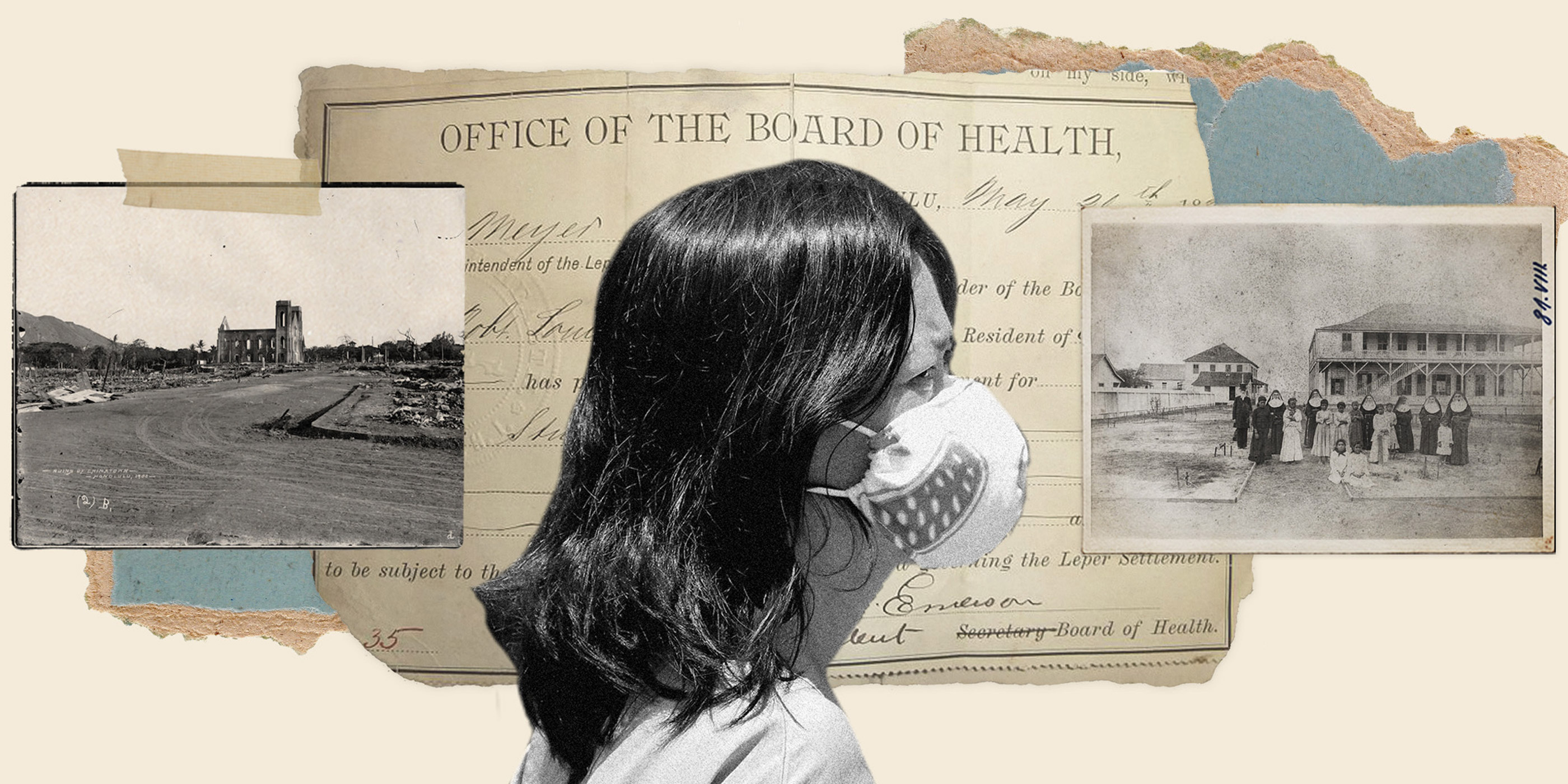
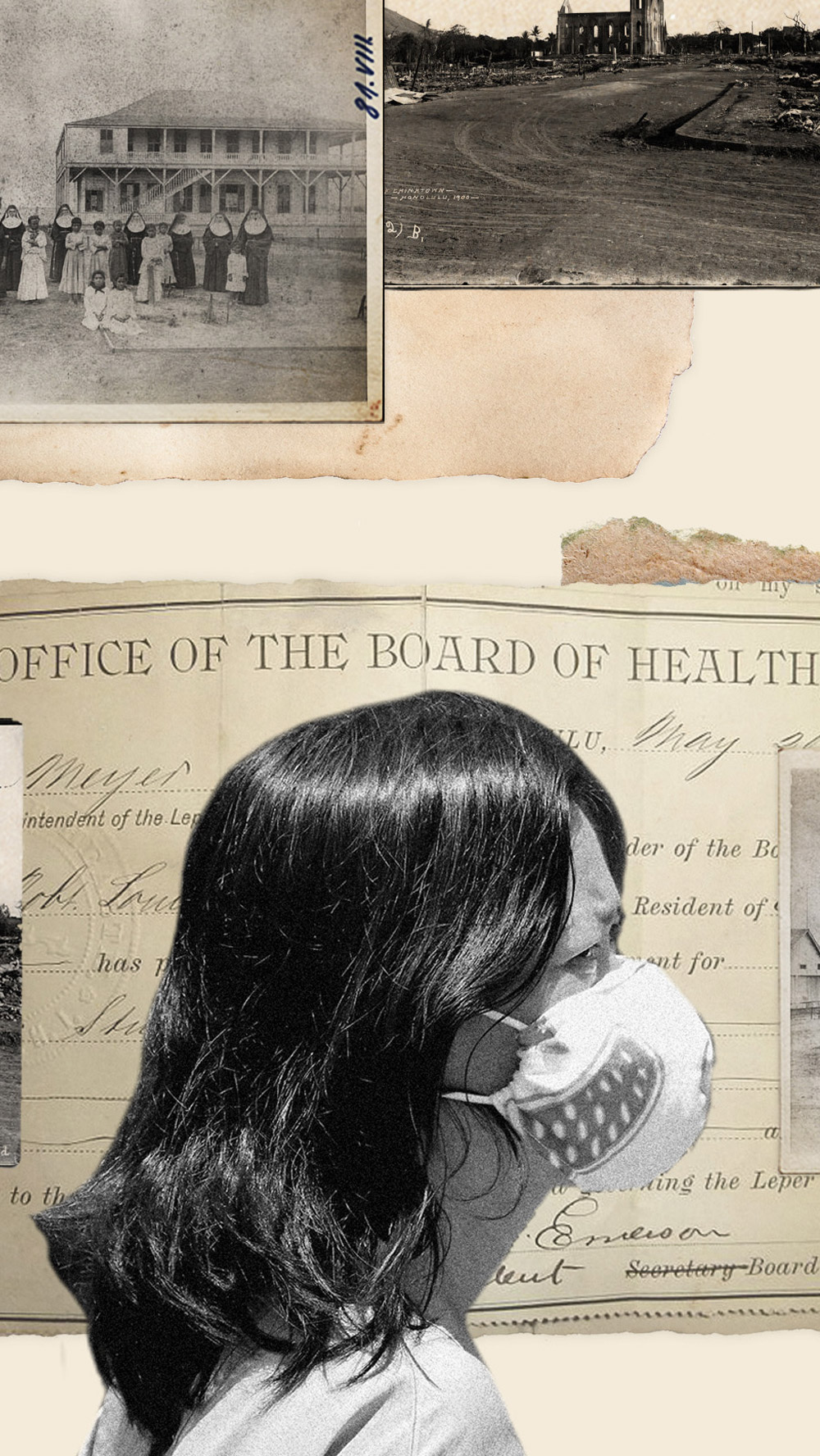
This isn’t the first time Honolulu’s Chinatown has experienced racism catalyzed by a public health crisis.The bubonic plague, believed to have originated in China, spread throughout the world and touched down on the islands at the end of the 19th century. During this time, Hawai‘i was a thriving economic hub in the Pacific Rim coming to terms with full colonial control and the 1893 overthrow of the Hawaiian monarchy. Eurocentric ideology was at a high, which helped foster blatantly racist and false ideas, such as the belief that the “plague seldom attacks clean white people,” as one Honolulu resident wrote.
Under economic pressure, officials first sought to quarantine Chinatown, a working class neighborhood made up of shanties and considered “dirty,” before resorting to burning down entire buildings where plague victims died as a method of “sanitation.” In early 1900, one of these fires burned out of control and swallowed a fifth of Honolulu’s buildings in flames. The residents of the homes that burned down were mainly Chinese, Japanese, and Hawaiian, who were then forced into quarantine camps for weeks with no proper compensation plan to help rebuild their lives.
This displacement of lower working class families, which would leave them struggling to catch up economically for years to come, was a result of public officials overlooking one of the most vulnerable and therefore least influential populations. This political inaction was illustrative of how a society entrenched in white supremacy and colonialism failed to protect the people not considered valuable — in this case, poorer people and people of color.
When considering the intersection of racism and infectious diseases in Hawai‘i, we can’t overlook the leprosarium on the secluded Kalaupapa peninsula on Moloka‘i, an island west of Maui. The highly stigmatized leprosy, or Hansen’s disease, was first diagnosed in the islands in 1848. Little was known about the disease, and it was believed to be more contagious than it actually is. But as with the bubonic plague in Honolulu’s Chinatown, racism infiltrated the way it was handled by public health officials.
From 1866 to 1969, over 8,000 people were permanently exiled to Moloka‘i for having leprosy. Those exiled were not only expected to die there, but society also shunned them as “impure” criminals simply for having the disease. About 97 percent of those exiled to the settlement were Native Hawaiian, a population already shrinking from other diseases introduced by European settlers, while foreigners with leprosy were reportedly allowed to leave the country. Although those exiled to the settlement were eventually given the freedom to return back to society, many found it difficult to be fully welcomed back, instead choosing to live out their lives on Moloka‘i. Today, researchers recall what happened on Moloka‘i to be an example of white colonist interest using public health discourse to segregate, tear apart, and ultimately disempower Native Hawaiian communities.
These examples are not isolated events, and they should not be forgotten. If we don’t learn from the past, we risk further harming groups of people who are already marginalized. In Hawai‘i, two populations especially vulnerable to the pandemic — the houseless and the incarcerated — are disproportionately made up of Native Hawaiian and Pacific Islander peoples. Although Native Hawaiians make up 24 percent of the state’s population, they account for 39 percent of the prison population.
This disproportionate representation shows up in our houseless population as well. In 2019, Hawai‘i ranked as the state with the second-highest rate of homelessness, and the majority of people who use homeless shelters are Native Hawaiian and Pacific Islander. It’s notoriously hard to make ends meet in Hawai‘i, where the cost of living is high, but the cycle of poverty is especially difficult for Native Hawaiians, who have been trying to recover ever since Europeans arrived. In 2017, the poverty rate for all Hawai‘i residents was 9.5 percent, but for Native Hawaiians, it jumped to 13.4 percent — the disparity likely due to lower education levels and lower wages.
In California, despite making up a small part of the state’s population, Native Hawaiians and Pacific Islanders have the highest COVID-19 death rate of any group. And these aren’t the only groups of people being affected at a disproportionate rate — Indigenous, Latinx, and Black communities are also suffering due to racial disparities in our health care system across the nation.
If this month serves any purpose, it is for everyone — not just those of API descent — to reflect on how racism itself is intertwined with systems of oppression. If the numbers above indicate anything, it’s that the harmful effects of colonialism and decades of systemic oppression are long lasting and impact countless aspects of many people’s lives. As a vehicle for racism, COVID-19 presents a critical lesson. This pandemic — and the others from Hawaii’s history — sheds light on the damaging legacy of racism and oppression. As health and safety are rightfully on people’s minds, it’s going to take everyone working together to forgo harmful, unproductive racist ideologies and instead advocate for our politicians and institutions to ensure that everyone feels protected and safe — now, and after the moment of crisis has passed.
Related Issues
Related Content
-
Press ReleaseJun 2026

Racial Justice
Civil Liberties
Aclu Reacts To Draft Bipartisan Ai Bill That Would Preempt State Laws. Explore Press Release.ACLU Reacts to Draft Bipartisan AI Bill That Would Preempt State Laws
WASHINGTON — Today, Congressman Obernolte and Congresswoman Trahan released a draft regulatory framework for Artificial Intelligence, which they may soon introduce in the House of Representatives. This draft bill – if enacted into law – would largely prohibit states from regulating AI developers. It would block states from enforcing existing state protections and from enacting new protections This could include anything from privacy regulations to antidiscrimination requirements to AI safety laws. Congress has twice overwhelmingly rejected legislative proposals to block states from regulating AI, also known as “preemption.” This includes a 99-1 Senate vote last year against an amendment that would have created a 10-year moratorium on state AI regulation. Seventeen Republican governors joined the bipartisan opposition to that failed amendment. In response, Jina John, senior policy counsel for AI, privacy and technology at the ACLU released the following statement: "This draft bill fails to learn from Congress’s previous attempts to block state AI regulations. States must be able to protect their own residents from harm, hold tech companies accountable, and ensure that AI is safe and trustworthy. "Governors, attorneys general, and lawmakers from both parties have opposed the efforts to push states aside for good reason. AI touches all aspects of people’s lives in this country, including employment, healthcare, lending, education, and so much more. So far, it has been governors and state legislatures—and largely not Congress or the president—who have been trying to protect the American people from harms that AI may cause. The federal government must not grant tech giants a blank check to deploy these technologies without the oversight of states." -
News & CommentaryMay 2026

Privacy & Technology
+2 Issues
Studies Question Value Of Ai-assisted Police Reports. Explore News & Commentary.Studies Question Value of AI-Assisted Police Reports
Researchers asked experienced police supervisors to rate police reports, some of which were written by humans and some by AI -
News & CommentaryMar 2026

Racial Justice
Pioneering Legal Advocate Pauli Murray Set The Blueprint For Aclu’s Racial Justice And Gender Equality Activism Today. Explore News & Commentary.Pioneering Legal Advocate Pauli Murray Set the Blueprint for ACLU’s Racial Justice and Gender Equality Activism Today
From dismantling ‘Jane Crow’ laws to advancing the rights of protesters, Pauli Murray’s legacy has paved the way for litigation, advocacy, and organizing. -
Press ReleaseFeb 2026
Racial Justice
Department Of Education Backs Down On Unlawful Directive Targeting Educational Equity. Explore Press Release.Department of Education Backs Down on Unlawful Directive Targeting Educational Equity
CONCORD, N.H. – In a victory for academic freedom and education equity, the U.S. Department of Education conceded the end of its February 14, 2025, “Dear Colleague” directive that sought to restrict diversity, equity, and inclusion (DEI) efforts in schools and higher education institutions nationwide. Upon the U.S.’s concession that the directive and subsequent certification requirement are vacated – meaning they are formally nullified – the district court issued a final ruling today, permanently invalidating the directive and preventing the government from enforcing, relying on, or reviving it. As a result, the challenged guidance is no longer in effect and cannot be enforced against anyone, anywhere nationwide. “This ruling affirms what educators and communities have long known: celebrating the full existence of every person and sharing the truth about our history is essential,” said Sharif El-Mekki, CEO at The Center for Black Educator Development. “Today’s decision protects educators’ livelihoods and their responsibility to teach honestly. At a time when many communities are facing severe teacher shortages, this signals that teachers can enter and stay in the profession, bringing their full selves to the classroom and fostering inclusive environments that prepare students for the future. “Across the country, educators do everything in their power to support every student, so each feels safe, seen, and is prepared for the future. Donald Trump and Linda McMahon tried to use politically motivated attacks and vague directives to stifle speech and erase essential teaching and learning in our schools and universities. The courts rejected that attack on public education. While Trump and McMahon want to ban diversity, equity, and inclusion, educators know these values are at the core of our nation. Diversity is our uniqueness and our strength. Equity means every student gets what they need, when they need it, and in the way that serves them best. And inclusion means all students are seen, valued, respected, and have access to opportunities and support,” said Becky Pringle, president at the National Education Association. "The Trump administration’s unlawful Dear Colleague Letter and certification requirement have now been vacated and abandoned, underscoring how badly Trump and McMahon overreached in their attempt to interfere with curriculum and instruction. Educators, parents, and community leaders will continue to organize, mobilize, and take action to protect our students and their futures." In an earlier ruling in the case, District Court Judge Landya McCafferty previously found that the directive’s “isolated characterizations of unlawful DEI” conflicted with the term’s meaning, stating that DEI is generally understood as fostering “a group culture of equitable and inclusive treatment.” The court further held that plaintiffs were likely to succeed in showing that the directive was vague, viewpoint discriminatory, and unlawfully imposed new legal obligations for educators and schools. “This ruling ensures that educators can engage in scholarship and teach history, literature, and other subjects where race, gender, and the values of diversity, equity, and inclusion appear, without fear of arbitrary or discriminatory enforcement, said Sarah Hinger, deputy director of the ACLU Racial Justice Program. “It affirms that educators must be free to teach and that students have a right to a full and honest education that reflects the diversity of their communities and prepares them to participate in our democracy.” "We are deeply grateful to the courageous NEA-New Hampshire member educators who stood up for their students and their profession by participating in this lawsuit. Their actions and the rulings from courts on this issue reaffirm that every student deserves the opportunity to learn in a school where they are valued, seen, and supported for who they are, not erased by political agendas. And their leadership sends a clear message that educators, not politicians, belong at the center of decisions about teaching and learning. We will continue to fight alongside our members for schools that serve all students,” said NEA-New Hampshire President Megan Tuttle. Gilles Bissonnette, legal director of the ACLU of New Hampshire, said, “Today is a victory for academic freedom, the free speech rights of educators, and for New Hampshire students who have a right to an inclusive education free from censorship. Every student, both in the Granite State and across the country, deserves to feel seen, heard, and connected in school – and that can't happen when classroom censorship laws and policies are allowed to stand." The lawsuit was filed last year by the American Civil Liberties Union, the ACLU of New Hampshire and the ACLU of Massachusetts on behalf of the National Education Association (NEA), and the National Education Association–New Hampshire. The Center for Black Educator Development as well as several New Hampshire School Districts later joined the case as plaintiffs.