How Nursing Homes Got Away With Hiding Bodies During the COVID-19 Outbreak


When COVID-19 first reached the U.S., the epicenter was a single nursing home in Washington State, where 45 people died. That nursing home outbreak was a precursor of what was to come. Ever since, the virus has been devastating nursing homes across the country, due in part to systemic mismanagement and discrimination against the people who live and work inside.
To date, deaths in nursing homes and other congregate care facilities account for almost half of all COVID-19 deaths in the country, despite these groups making up less than 1 percent of the population. Residents of these congregate facilities are dying from COVID-19 at 8.6 times the rate of the overall 75+ population.
If current trends hold, that means nearly 90,000 people living in nursing homes and other congregate care settings could die by October 1.Grim as this projection is, the actual death toll to date is likely much higher than currently reported. It took the Department of Health and Human Services (HHS) months after declaring COVID-19 a national emergency to start requiring nursing homes to report deaths and infections despite ample evidence that these facilities were at high risk. Even now, nursing homes are only required to report data from May 8 onward. HHS doesn’t require other congregate settings for people with disabilities, such as psychiatric homes, to report at all. This lack of transparency, in addition to the government’s systemic mismanagement of nursing homes and other congregate settings, has helped create the crisis we see today. In some cases, facilities have not only failed to report, but have actively hidden deaths from residents, families, and the government. For example, a nursing home in the Harlem neighborhood of New York City hid 26 COVID-related deaths from the state by covertly shipping bodies out of the facility. At a nursing home in New Jersey, 17 bodies were packed into a shed and later crowded into a morgue meant to house only four bodies. Other stories emerged of residents’ families being left in the dark about whether loved ones were dead or alive.
While HHS has lagged in collecting data, states can independently choose to require reporting and publicize this information. But too often, states are slow to report, and the data is often piecemeal and insufficient for analyzing the full scale of the pandemic.
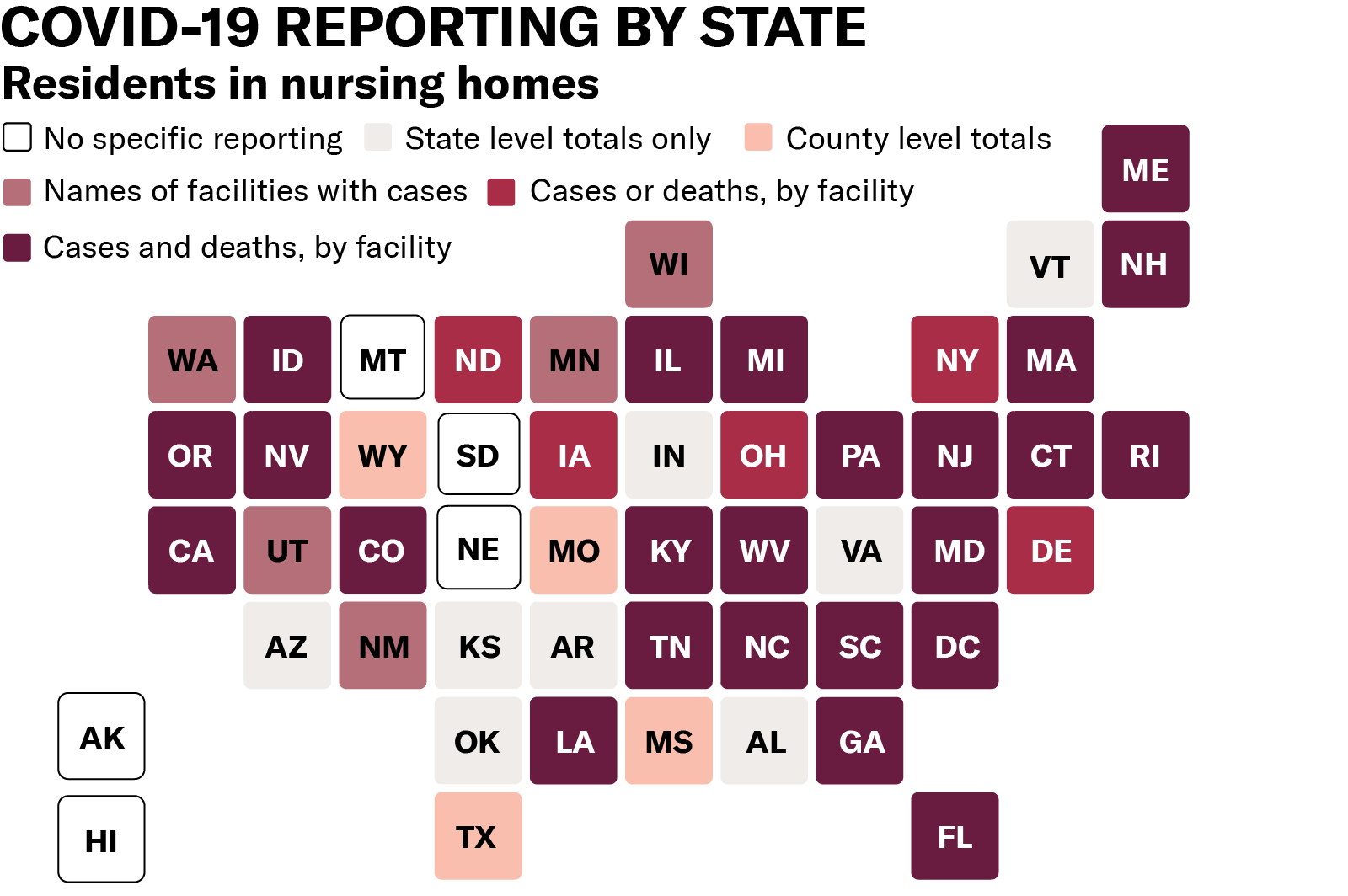
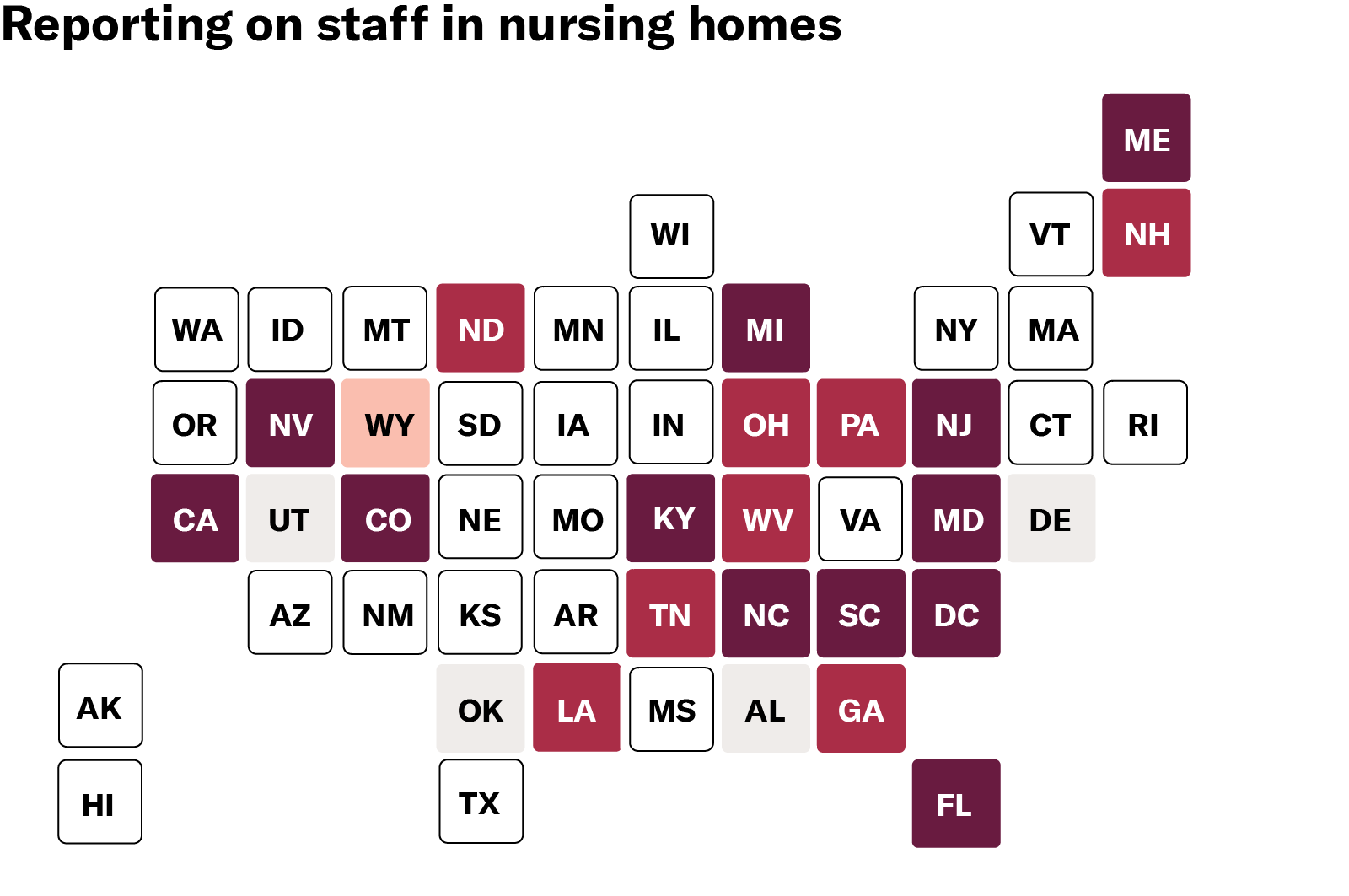
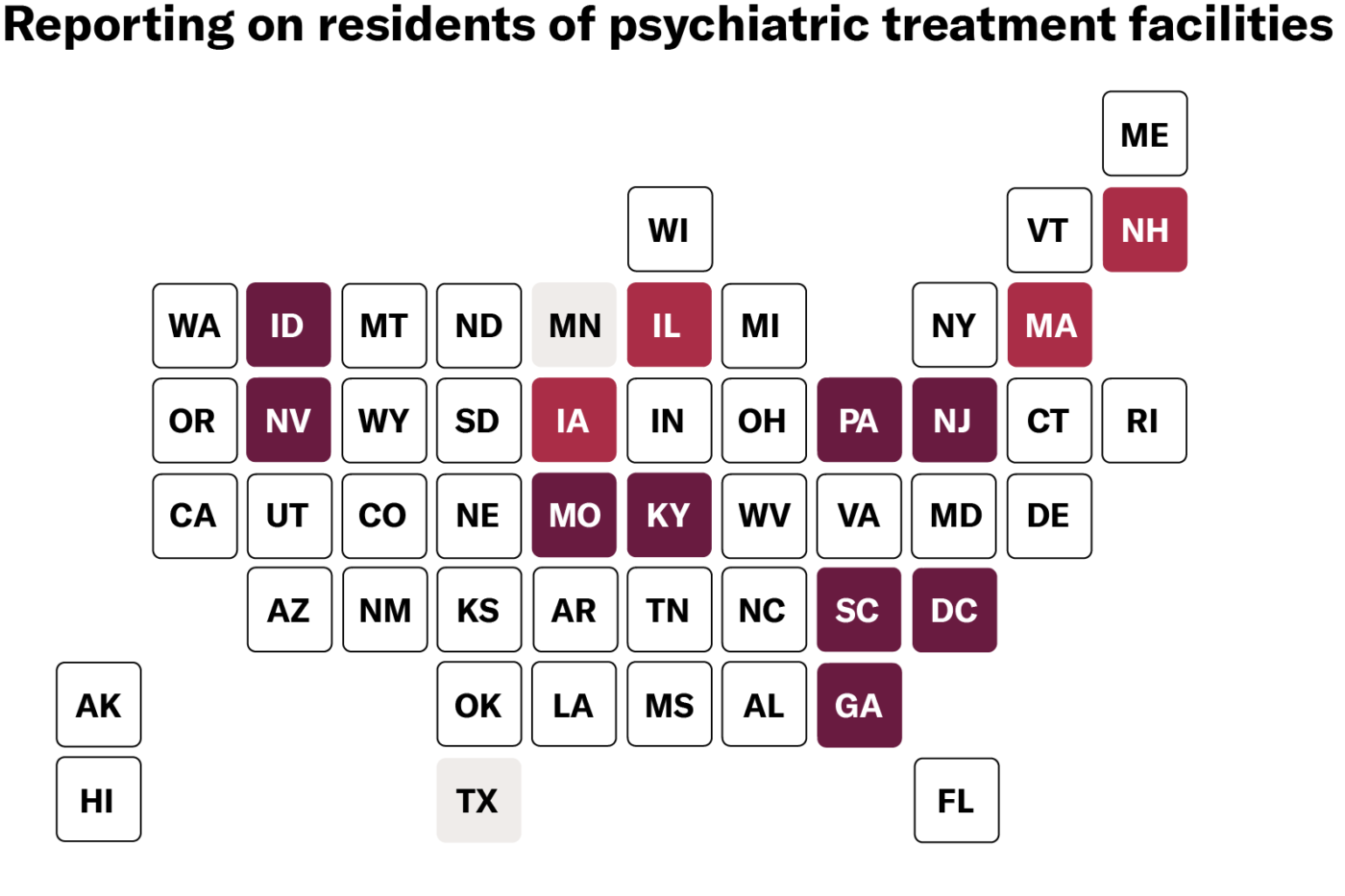
As of June 29, only 41 states report deaths in nursing homes, and the level of detail varies from state to state. Some states offer only state or county totals (such as Arkansas, Indiana, Vermont, and others) while others break down data by facility (including North Carolina, West Virginia, and Nevada). Only 12 states go as far as naming facilities, reporting both cases and deaths, and disaggregating between residents and staff. Disaggregating data in this manner allows us to more accurately measure the impact on various groups of people. Residents are mostly seniors and all are people with disabilities. Staff are disproportionately people of color, women, and low-income. All of these demographic variables are relevant and integral to any adequate public health response. Even when states do report deaths and infections in nursing homes, most do not offer critical demographic data. This information is essential for assessing the impact of COVID-19 on different communities and demographic groups and facilitating our response. Yet only two states — Mississippi and Iowa — report the demographics of residents or staff who have tested positive or died. People with disabilities and the people who work with them deserve to be counted. States can and should modify current policies to collect and publicize vital data while maintaining privacy standards. Last week, the ACLU filed a petition calling on HHS to do its job to address this crisis — and its job includes collecting and reporting full data from facilities that receive Medicaid or Medicare dollars.The government needs good data to adequately respond to COVID-19. Data helps to inform where to investigate, where to channel resources, and what policies and practices to adopt. At the individual level, data helps people decide which facilities to live in and which to avoid. And in the long run, data can propel change to ensure this crisis never happens again.
The first step to change the system is to get to the truth. HHS must tell the truth about what is happening in the nursing homes and other congregate settings for people with disabilities that it oversees and funds with our taxpayer dollars. Maps reflect public data reporting as of 06/29/2020. Links to state-level data sources available here.
This piece is part of a series, read the previous entry here:

COVID-19 Deaths in Nursing Homes are Not Unavoidable — They are the Result of Deadly Discrimination
We as a society must reckon with our relentless marginalization and de-prioritization of people with disabilities and the people who support them.
Source: American Civil Liberties Union
Related Issues
Related Content
-
News & CommentaryJul 2026

Disability Rights
Bans On Lifesaving Program For People Who Use Illegal Drugs Violate The Americans With Disabilities Act. Explore News & Commentary.Bans on Lifesaving Program for People Who Use Illegal Drugs Violate the Americans with Disabilities Act
Syringe Service Programs provide access to crucial health services to people with substance use disorders. The ACLU is fighting against bans that limit these lifesaving programs. -
Press ReleaseJul 2026

Disability Rights
People With Disabilities, Advocates Sue City Of Portland And Multnomah County Over Inaccessible Emergency Systems. Explore Press Release.People with Disabilities, Advocates Sue City of Portland and Multnomah County Over Inaccessible Emergency Systems
PORTLAND, Ore. — People with disabilities and disability rights advocates have filed a federal lawsuit against the city of Portland, Multnomah County, and their top elected officials, alleging that the jurisdictions' emergency management systems fail to protect people with disabilities before, during, and after disasters — in violation of the Americans with Disabilities Act (ADA), Section 504 of the Rehabilitation Act, and Oregon law. “Five years ago, as temperatures soared above 115 degrees, far too many disabled Portland residents could not reach cooling centers or even access usable emergency information. As a result, people with disabilities were overrepresented among those who died,” said Malhar Shah, senior staff attorney with the ACLU Disability Rights Program. “With the threat of extreme weather and disasters like wildfires only accelerating, Portland and Multnomah County have a legal duty to make their emergency system accessible to people with disabilities and give them the equal opportunity to survive.” The complaint seeks to avoid a repetition of the city of Portland and Multnomah County's response to the June 2021 extreme heat wave, when temperatures reached an all-time high of 116 degrees and 69 people died of heat-related causes in Multnomah County — with people with disabilities overrepresented among the dead. Many victims lived on upper floors of multi-family housing, in trailers and RVs, or were unhoused. Survivors with disabilities reported being unable to reach cooling centers, obtain accessible transportation, or access timely, usable emergency information. That risk is not abstract. A local wildfire expert who studied the 2025 Eaton Fire in Los Angeles — which killed at least 17 people and destroyed 9,000 structures — found that Portland is less prepared and has fewer resources than Los Angeles did before that disaster. Forest Park has only two wildfire-detection cameras, and Southeast Portland's Oaks Bottom area, where three fires have already ignited this year, has none at all. “We’re in a wildfire emergency right now statewide and people with disabilities cannot be an afterthought,” said Jake Cornett, executive director at Disability Rights Oregon. “We often hear about victims with disabilities in the aftermath of disasters — and that’s not good enough. We need the city and county to have an inclusive plan to evacuate and shelter people with disabilities long before a wildfire, flood, earthquake, or some other disaster strikes.” The lawsuit was filed by Disability Rights Oregon, Disability Law United, the American Civil Liberties Union, and law firm Cambreleng & Marton, and names the City of Portland, Multnomah County, Portland Mayor Keith Wilson, and Multnomah County Board Chair Jessica Vega Pederson as defendants. Plaintiffs in the lawsuit are Disability Rights Oregon, Oregon’s federally designated protection and advocacy organization, and Bridges Oregon, a nonprofit that serves Deaf, DeafBlind, Hard of Hearing, and Late-Deafened Oregonians. Three individuals also join the case: Audra Pearson, a Portland resident with cerebral palsy who relies on a powered wheelchair, paratransit, and round-the-clock caregiver support: “I can't just grab a bag and walk out the door during an emergency — I need an accessible vehicle, a shelter that fits my wheelchair, and staff who know how to help me. Nobody has ever asked what I'd need to survive a disaster, even though it's obvious I'd need help. That has to change before it costs someone their life." Jonathan Simeone, a Portland homeowner who is blind: “Learning about the emergency system created and maintained by Portland and Multnomah County, I realized they do not include those of us with disabilities in their emergency planning and that their violations of our civil rights have resulted in those of us with disabilities being more likely to suffer injury or death during an emergency simply because we are disabled and Portland and Multnomah County have not considered the rights of disabled people with the care they have considered the rights of nondisabled people." Philip Wolfe, a Deaf Portland resident: "I have the same right to survive a disaster as anyone else, but every time there’s a wildfire, heat wave, or other dangerous emergency, I worry whether I'll get the information I need in time.” The lawsuit alleges that Portland and Multnomah County's emergency system denies people with disabilities meaningful access at every phase of disaster response: Alerts and warnings are shared in inaccessible formats, including maps without descriptive text and social media videos without captions or ASL interpretation. Evacuation assistance is unreliable: the city and county have no adequate way to identify residents who need help, lack accessible vehicles and trained drivers, and exclude entire categories of residents with disabilities — including people in high-rises, psychiatric facilities, and group homes — from evacuation plans altogether. Shelters and recovery centers are riddled with known accessibility barriers, and there is no concrete plan to fix them or to ensure access to medication and equipment after a disaster. Planning, training, and outreach continue to exclude the disability community, despite years of advocacy and documented requests to be included. “This isn't a case of a government caught off guard,” said Ayelet Weiss at Disability Law United. “The City's own auditor and community members have urged the Defendants to include individuals with disabilities in a comprehensive planning process for years. That hasn't happened, and the needs of the disabled go unaddressed. As the City Auditor put it, ‘This lack of preparation puts the lives of people with disabilities at risk.’” The lawsuit asks the court to declare that Portland and Multnomah County's emergency planning, preparedness, response, and recovery programs violate the ADA, Section 504, and Oregon law; order the city and county to design, implement, and maintain an emergency management system — covering alerts, evacuation, shelter, and planning — that is fully accessible to people with disabilities; and award damages to individual plaintiffs and reasonable attorneys’ fees and costs to organizational plaintiffs. “When the law is ignored for years, litigation is the necessary next step to ensure equal protection for all Oregonians,” said Rebecca Cambreleng, partner at Cambreleng & Marton and co-counsel on the case. “We intend to see this through until the city and county meet their legal obligations to everyone with disabilities.” Plaintiffs tried to resolve these issues without litigation by notifying the city and county of their findings in February 2025 and meeting with counsel in March 2026. After those efforts failed to produce meaningful commitments, plaintiffs notified defendants of intent to sue in June 2026. The complaint is available here: https://www.aclu.org/cases/simeone-v-multnomah-county?document=Complaint -
OregonJul 2026

Disability Rights
Simeone V. Multnomah County. Explore Case.Simeone v. Multnomah County
-
Press ReleaseJun 2026
Disability Rights
Aclu Statement On Doj Memo Threatening The Right To Community Living For People With Disabilities. Explore Press Release.ACLU Statement on DOJ Memo Threatening the Right to Community Living for People with Disabilities
WASHINGTON – The Department of Justice’s Office of Legal Counsel (OLC) has issued a memorandum that incorrectly purports that neither federal disability rights laws nor Supreme Court precedent enshrine the right of people with disabilities to live integrated lives in their communities, instead of being segregated in institutions. Zoe Brennan-Krohn, director of the Disability Rights Program at the American Civil Liberties Union, had the following response: “Trump’s Justice Department cannot erase federal laws and decades of legal precedent with a single opinion. The memo itself acknowledges it is ‘out of step’ with longstanding and consistent federal court opinion interpreting what the Americans with Disabilities Act and Section 504 of the Rehabilitation Act require, but it is far worse than that. This is a blatant attempt to undermine the rights of disabled people. “Nearly three decades ago, the Supreme Court in Olmstead v. L.C. recognized a ‘right to live in the world,’ and also recognized that state and local governments have an obligation to end the long and dark history of segregation and institutionalization of disabled people. Olmstead confirmed that disability rights laws require states to provide people with disabilities with services in an integrated manner in the communities. For far too long, disabled people faced neglect, isolation, and inhumane conditions in institutions. Olmstead made clear that this segregation must end. “The DOJ’s statement is wrong on the law, and does not change the rights of disabled people. The right to live in the community is foundational to disability rights law. We won’t stop fighting to protect it.”